
Ankle sprains are THE most common injury in the sporting world.
In a significant number of people, up to 30% in some studies, there are ongoing issues with the ankle after a sprain: this means that people do not fully recover after injury. They often complain of pain and swelling and have a sense of insecurity or even frank instability. This means that the ankle may roll with even relatively simple every day activity.
In general terms, treatment for an ankle sprain should initially be RICE
Rest
Ice
Compression
Elevation
Physiotherapy can be of help but should not continue for an indeterminate period. You should find relatively rapid improvement after an ankle sprain. If you feel that you are not progressing quickly after such an injury and especially if you feel that you are not improving on an ongoing basis, then the matter should be reviewed by a sports physician or a GP with an interest in sports medicine.
It has been my experience that, by 3 weeks after an ankle sprain, you should be progressing rapidly and be back to most everyday activities. If not, then you should consider seeking an opinion from a professional such as a sports medicine doctor or Orthopaedic surgeon, such as A/Prof Miniter.
A note of treatment recommendations and the need for accurate diagnosis by a doctor trained appropriately for this purpose.
Practitioners other than doctors are not trained to make diagnoses with a balanced assessment of history, physical examination and then interpretation of investigations as needed. Be careful to avoid definitive treatment recommendations from those that are not trained to make these decisions, which, after all, are very important and may directly affect your health. You need to see someone who is properly trained to make these diagnoses accurately. It is most effective and the least time consumptive and financially efficient route to obtain a definitive opinion at the outset. This saves a great deal of expense, frustration and misdiagnosis.
Reasons for not improving:
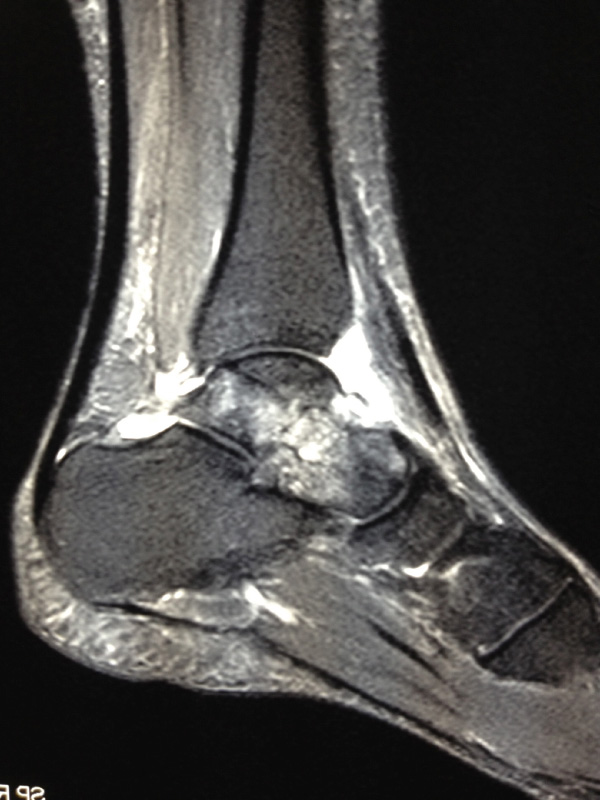
If you are not improving quickly, then we may need to evaluate the ankle by examination and MRI scanning and XRay. The following may be issues that require diagnosis and treatment:
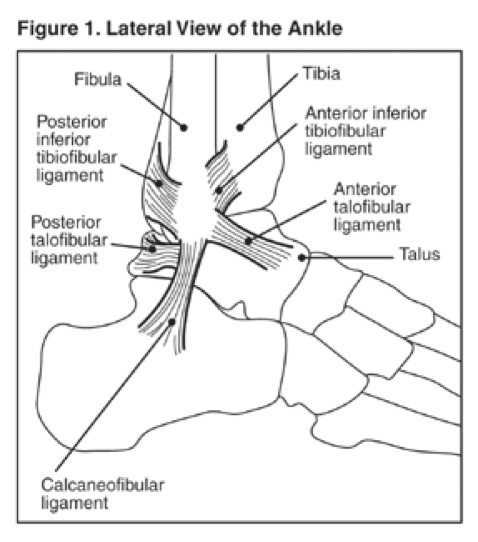
Instability— Lateral:
The lateral ligament of the ankle is actually 3 ligaments but only 2 of them are commonly injured: The ATFL and the CFL. If they heal in an elongated condition, then the ankle is unstable. This may present as a feeling of insecurity over uneven ground or perhaps even episodes where the ankle rolls. This can occur with very little trauma and can lead to a fall or an inability to return to sports. It can be dangerous if you lose your footing, falling heavily. It is not just the province of the young: older folk are sometimes more significantly affected by ankle instability than the young.
Where the ankle is unstable, A/Prof Miniter may well recommend a reconstruction, a procedure where the ligaments are identified (they are still there and waiting to be repaired) and then brought back to their original position. This is a simple procedure, usually combined with an arthroscopy and is followed by a very short period of immobilisation.
Recovery after ankle reconstruction:
Crutches are used for 3 to 5 days; we then remove the plaster, provide you with a walking boot and resume full weight bearing in most cases. The boot is to be discarded by 2 or 3 weeks at most. Physiotherapy, EP and hydrotherapy are started very soon after the surgery, often after just a week or so.
We will usually recommend that you start walking normally around the home without the boot in the first week after the surgery. The boot is then to be used for longer journeys such as for a trip to the shops.
We would expect that you will take a short period of time away from work and that you rest at home with ice and elevation for the first week or so. This allows the wounds to heal and the swelling to be kept well under control.
Return to full sporting activity will require 3 months or so. Lesser everyday activities require 3 to 6 weeks or less. Most people are surprised by the speed at which they return to functional tasks.